Key Highlights
First-of-its-kind study to examine outcomes, evaluate analytics, identify barriers/challenges, analyze performance improvement processes, and identify opportunities for future research.
Sites collected qualitative and quantitative data on 10 AONN+ evidence-based navigation metrics. Validated evidence-based tools were incorporated into the study design for data collection to help ensure like data elements were captured across study sites.
| Domain | Metric |
|---|---|
| Care Coordination/Care Transition | Barriers to care; measuring the number and list of specific barriers to care identified by navigator per month |
| Care Coordination/Care Transition | Diagnosis to initial treatment; measuring the number of business days from diagnosis (date pathology results obtained) to initial treatment modality (date of 1st treatment) |
| Operations Management/Organizational Development/Health Economics | Navigation caseload; measuring the number of new cases, open cases, and closed cases navigated per month |
| Operations Management/Organizational Development/Health Economics | Measuring the number of navigated patients readmitted to the hospital at 30, 60, and 90 days |
| Psychosocial Support Services/Assessment | Psychosocial distress screening; measuring the number of navigated patients per month who received psychosocial distress screening at a pivotal medical visit using the National Comprehensive Cancer Network distress screening tool |
| Psychosocial Support Services/Assessment | Social support referrals; measuring number of navigated patients referred to support network per month |
| Survivorship/End of Life | Palliative care referral; measuring number of navigated patients per month referred for palliative care |
| Patient Advocacy/Patient Empowerment | Identify learning style preference; measuring the number of navigated patients per month whose preferred learning style was discussed during the intake process. The group agreed this should be included, if we can identify a validated tool |
| Professional Roles and Responsibilities | Navigation knowledge at time of orientation; measuring percentage of new hires who have completed institutionally developed navigator core competencies |
| Research/Quality/Performance Improvement | Patient experience/patient satisfaction with care; measuring patient experience or patient satisfaction survey results per month. The group determined use of CCHAPS (Community-wide Children’s Health Assessment & Planning Survey) for measuring patient satisfaction |
Study demographics include 2 academic, 2 community, 2 Oncology Care Models, and 2 maturing programs each with with more than 750 analytic cancer cases per year.

Performance Improvement
- Navigators play an instrumental role in identification of gaps in care and facilitation of performance improvement methodologies to drive practice change and quality
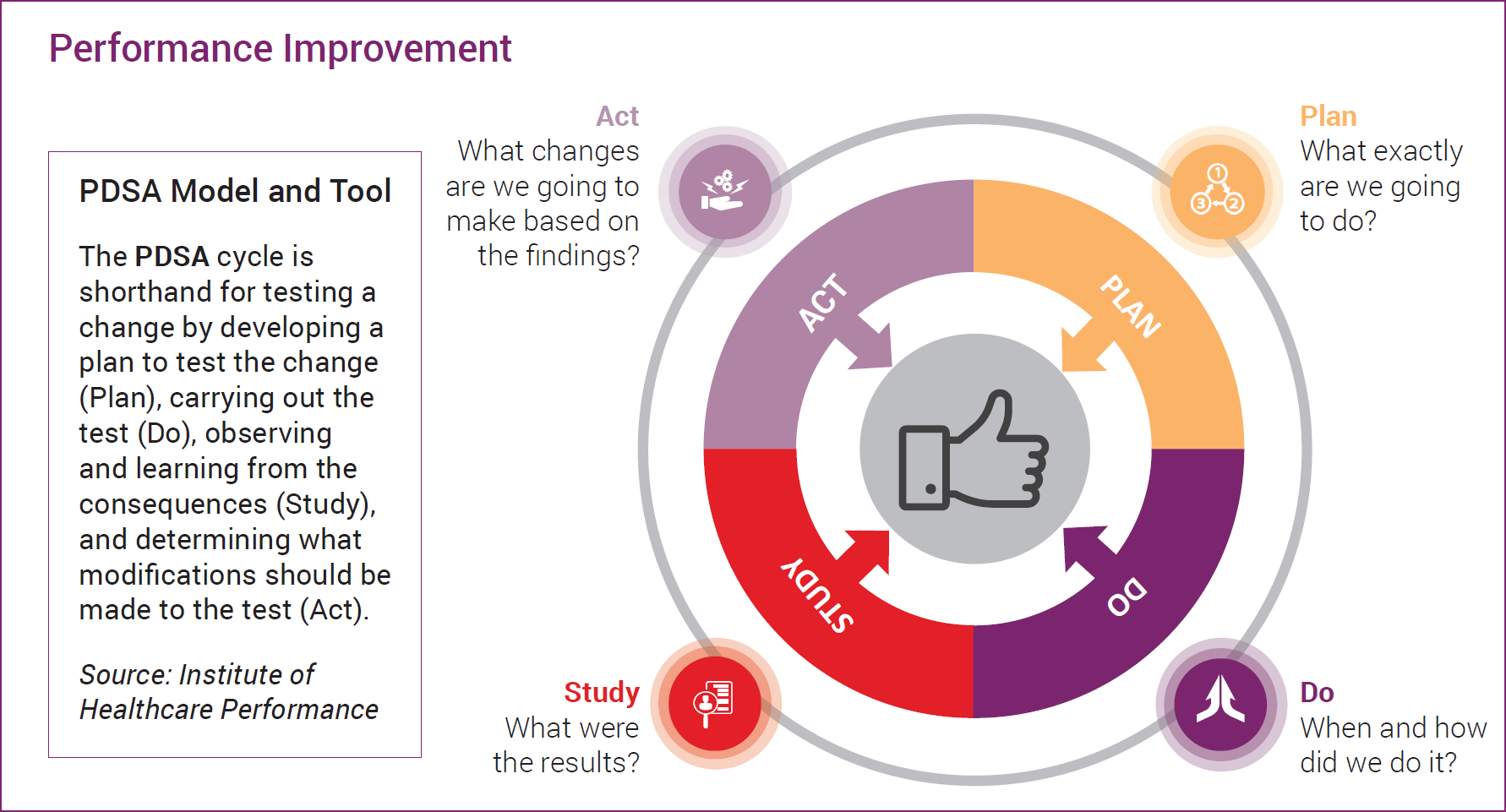
- Performance improvement studies were completed utilizing the PDSA model and template
- During the study period, sites conducted performance improvement activities in Distress Screening (4 sites), Palliative Care (4 sites), Patient Experience Survey (2 sites), and Caseloads (2 sites)
Case Example
Performance Improvements: Palliative Care
Measure Description
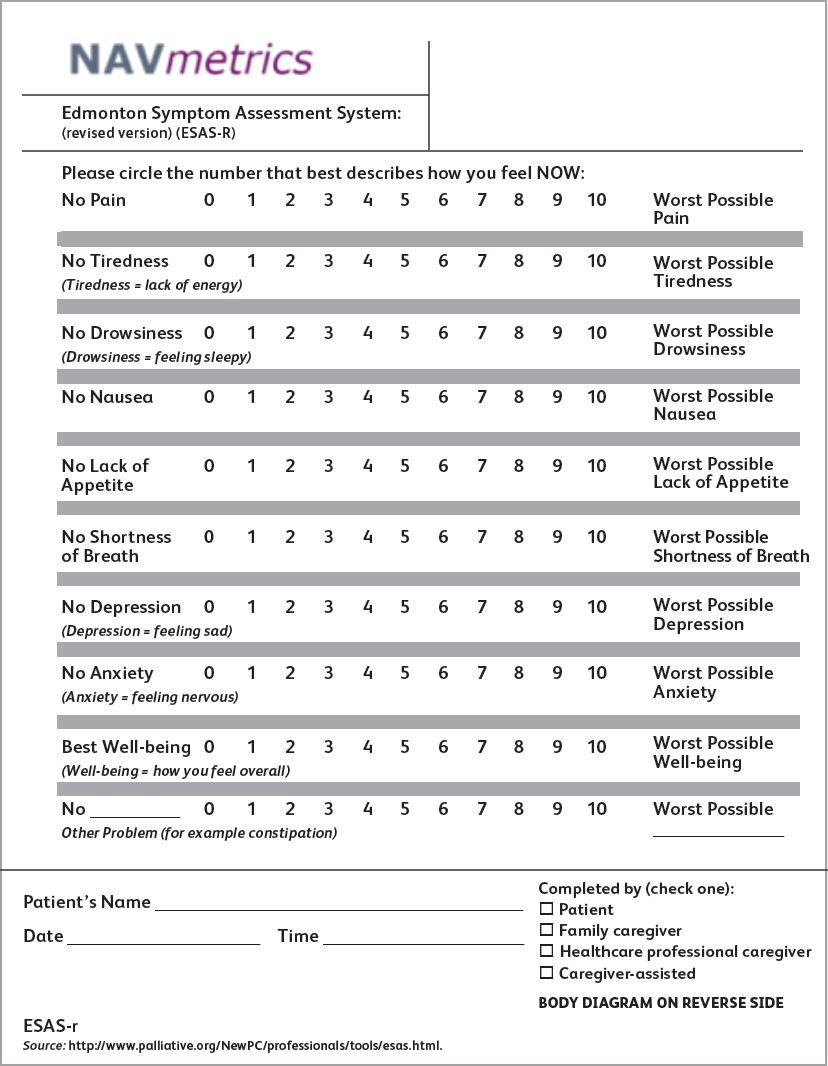
Number of navigated patients per month referred for palliative care services (for symptom management) utilizing a validated tool (ESAS, Edmonton Symptom Assessment System)
Opportunities
- Develop a formal process to assess patients
- Start with patients with advanced disease
- Determine best time frame for assessing patients
- “We never assessed our patients before palliative care needs”
Outcomes:
- Increase referrals to palliative care
- Our team found value in system assessments of our patients
- Proactive assessments for palliative care
- Nurse navigator completed with the patient and shared results “real time” with the physician